Implant placement in a patient with chronic periodontitis
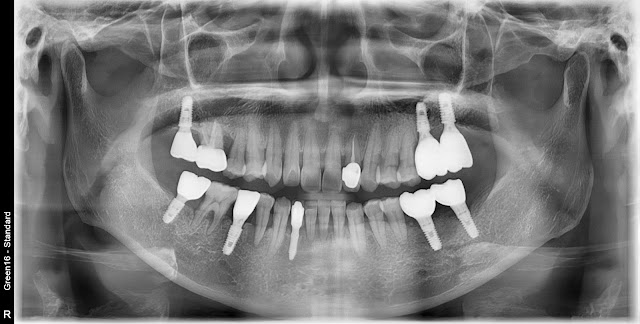
A 59-year-old female patient, immediate implant placement is planned for the site of tooth #46. The tooth was extracted due to severe tooth mobility caused by chronic periodontitis. There is partial loss of alveolar bone on the adjacent side, but it doesn't appear to be severe. An implant was placed, and Collacera was grafted in the gap area. A bone healing abutment was attached. Periopack was placed in the upper area. This is a postoperative radiograph. This is the final restoration photo approximately 4 months after the surgery.


